100 Plus Your Age, and other things we once believed
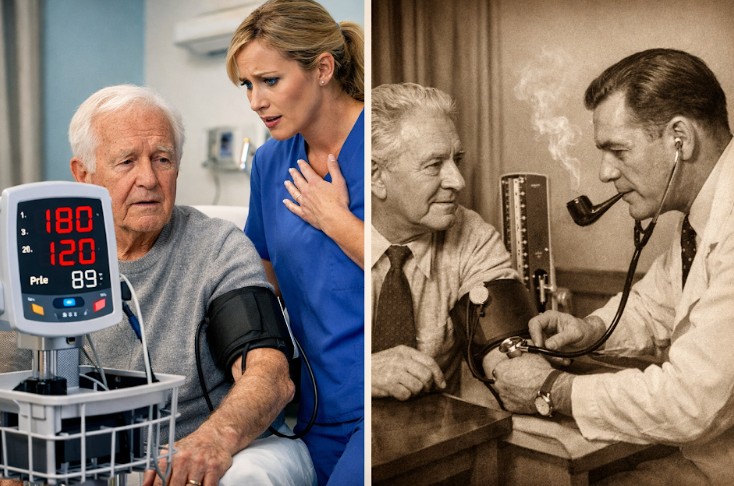
There was a time, not so very long ago, when a doctor might look at your blood pressure, nod thoughtfully, and say something along the lines of, “Well, that’s about right for your age.” 
The rule of thumb was simple enough to remember and reassuring enough to repeat: take your age, add one hundred, and that was your systolic blood pressure. A man of sixty could stroll around quite contentedly with a systolic blood pressure of 160, and no one would feel especially alarmed.
I first heard this sometime around 1975, and even then it already had the faint smell of something inherited rather than discovered, like an old piece of furniture passed down through generations of medical teaching. The instructor who mentioned it may well have been trained twenty or thirty years earlier, at a time when this was not merely a rule of thumb but something close to orthodoxy.
 It is easy now to look back and wonder how such a notion survived as long as it did, but medicine, like most human enterprises, does not update itself overnight. Ideas linger, particularly when they seem to fit everyday experience. If older people tended to have higher blood pressure, and many of them appeared to get on perfectly well, then perhaps that was simply how the body aged. It was a tidy explanation, and tidy explanations have a habit of sticking around.
It is easy now to look back and wonder how such a notion survived as long as it did, but medicine, like most human enterprises, does not update itself overnight. Ideas linger, particularly when they seem to fit everyday experience. If older people tended to have higher blood pressure, and many of them appeared to get on perfectly well, then perhaps that was simply how the body aged. It was a tidy explanation, and tidy explanations have a habit of sticking around.
My own family history offers a rather less tidy version of events. I was born in 1951, my mother’s first child, and her pregnancy was complicated by severe preeclampsia. Preeclampsia, for those who have not encountered it, is a condition of pregnancy marked by high blood pressure and signs that organs—particularly the kidneys—are under strain, often detected by protein in the urine. In severe cases it can progress rapidly and become life-threatening for both mother and child. My mother told me later that she nearly died, and given the state of obstetric care at the time, and the fact that my mother was herself an experienced midwife, that was not an exaggeration for dramatic effect but a fairly plain statement of fact.
She survived, had three more children, and for the rest of her life took blood pressure medication known then as Methyldopa, or Aldomet as it was commonly called.
It was, for its day, a modern drug. Introduced in the 1960s, it worked not by forcing the blood vessels open directly but by acting on the brain to reduce the signals that kept blood pressure high. It was particularly valued in pregnancy, which suggests that my mother, in a roundabout way, was receiving treatment at the forefront of what was then available. She remained on it for decades, lived to the age of seventy-eight, and eventually died of a stroke. Her father, I should add, died of a stroke at forty-nine, which suggests that whatever else was going on, there was a certain family tendency in that direction.
What is striking, looking back, is the coexistence of two ideas that do not sit comfortably together. On the one hand, there was a general acceptance that blood pressure rose with age and did not necessarily require intervention. On the other, there was a clear recognition that in certain circumstances, such as pregnancy, high blood pressure was immediately dangerous and demanded treatment. It was as if the medical profession had one foot in the world of benign neglect and the other in the world of urgent action, without fully reconciling the two.
The shift came gradually, and not without resistance. Long-term population studies began to accumulate evidence that higher blood pressure was not simply a feature of aging but a contributor to strokes, heart attacks, and all the other unwelcome developments that tend to arrive without invitation.
The most influential of these was the Framingham Heart Study, launched in 1948 by the U.S. Public Health Service in collaboration with what is now Boston University. It began with just over 5,000 residents of a single town, Framingham, Massachusetts, and followed them over decades, later adding their children and grandchildren. What made it so persuasive was not a single dramatic finding, but the slow accumulation of consistent evidence over time. By tracking ordinary people through the course of their lives, it became clear that elevated blood pressure, even when long tolerated, was strongly associated with later strokes and heart disease.
By the 1980s and 1990s, the idea that a systolic reading of 160 might be “normal for your age” had largely been abandoned, replaced by a more proactive approach that sought to reduce those numbers rather than accommodate them.
Living in Cuenca adds a small local twist to the story. At an altitude of around 2,500 meters, the air contains roughly the same proportion of oxygen as at sea level, but the pressure is lower, so each breath delivers less oxygen to the bloodstream—effectively the body is working with about three-quarters of the oxygen availability it would have at sea level.
Visitors often notice that their pulse is higher and their breathing a little more labored for the first few days. Blood pressure can also behave differently, although not always in predictable ways. There is a tendency to assume that everything should be adjusted upwards for altitude, just as it once was for age, but the evidence does not really support a simple formula. Long-term residents adapt, and whatever adjustments the body makes are not an excuse for allowing blood pressure to drift into the sort of territory that used to be waved through with a reassuring smile.
One occasionally hears modern variations on the old theme. Someone will say that a slightly higher pressure is acceptable “at your age,” or that there is no need to worry unless it is very high. There is a grain of truth in this, in the sense that treatment decisions are always individual, but it carries an echo of that earlier, more relaxed era. The difference now is that we have the benefit of hindsight, and hindsight, as usual, is less forgiving than contemporary opinion.
From the vantage point of a long life, and a career spent in healthcare administration, what stands out is not that people were careless or uninformed, but that they were working with the best understanding available to them at the time. The rule of “100 plus your age” was not invented out of laziness; it was an attempt to make sense of patterns that had not yet been fully explained. The trouble was that it made those patterns look more harmless than they really were.
If there is a lesson in all this, it is perhaps that the human body keeps score over decades, not days. A blood pressure that seems acceptable this year may not look quite so benign twenty years later, when the cumulative effect has had time to declare itself. My mother’s long course of treatment, her survival after a dangerous pregnancy, her father’s early death, and her eventual stroke were probably all elements marked on that same scoresheet.
_________________
This article reflects personal experience and general historical context rather than medical advice. Anyone concerned about blood pressure or medication should consult a qualified physician, particularly as modern treatment options and recommendations may differ significantly from those described here and treatment should be based on an individualized medical history, examination, and care plan carried out by a qualified professional.




")