






Why we’re not facing another 1918 epidemic

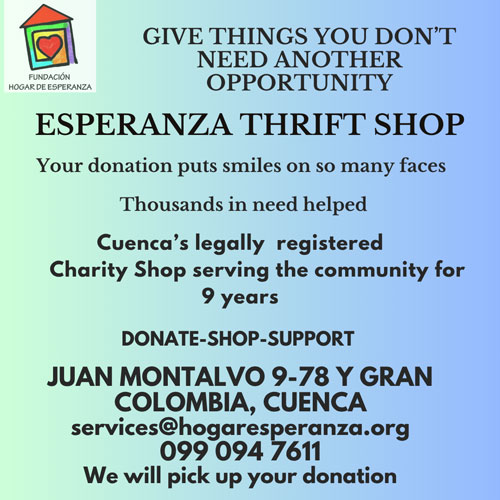
A ward of 1918 influenza patients at a U.S. armory.
By Jeremy Brown
We have just commemorated the centenary of the Great Flu Pandemic of 1918, which lasted only a few months but claimed 50 million to 100 million lives worldwide, including 675,000 in the United States. That pandemic remains a benchmark, and many![]() commentators have rushed to compare it to the current coronavirus outbreak. What’s most striking about these comparisons, though, is not the similarities between the two episodes, but the distance that medicine has traveled in the intervening century. Whatever happens next, it won’t be a second 1918.
commentators have rushed to compare it to the current coronavirus outbreak. What’s most striking about these comparisons, though, is not the similarities between the two episodes, but the distance that medicine has traveled in the intervening century. Whatever happens next, it won’t be a second 1918.
That year, as pandemic influenza ravaged communities as diverse as California and Kolkata, no one knew what was killing them. Theories abounded. Some suggested it was a misalignment of the planets. (That’s what gave us the name influenza, from the Italian word for “influence.”) Others believed the cause was tainted Russian oats, or volcanic eruptions. Microbiologists focused on a bacterium they had discovered decades earlier in the lungs of influenza victims, and called it Bacillus influenza. But they had merely recognized a bacterium that invades lungs already weakened from influenza. Not until 1933 did two British scientists demonstrate that the cause must be a new class of disease, which today we call viruses. Finally, in 1940, the newly invented electron microscope took a picture of the influenza virus, and for the first time in history we could not only name, but also see, the culprit.
The contrast with the coronavirus, which causes the disease COVID-19, could not be greater. From the very start of the outbreak, scientists suspected a virus. Within two weeks, they had identified it as a coronavirus, sequenced its genome, and discovered that the most likely animal hosts were bats. This information, which was published by a Chinese team, was instantly shared across the scientific community, allowing research labs around the world to begin the long and complicated process of understanding the virus, and finding a vaccine and a cure. We may not have beaten the enemy yet, but we certainly know a great deal about him.
The Great Influenza Pandemic of 1918 occurred in the pre-antibiotic era. Although antibiotics do not treat viruses, they do treat the secondary bacterial infections that sometimes follow. These secondary infections cause severe pneumonia, and were likely responsible for most of the deaths in 1918. Back then, there was little to offer. Physicians recommended quinine (not helpful), dry champagne (ditto, though more fun), and phenolphthalein (a cancer-causing laxative). During an earlier outbreak of influenza, in 1916, British military physicians had even tried bloodletting as they treated dying soldiers. When it failed, they suggested it had simply not been tried soon enough in the course of the disease. Patients survived in spite of their doctors.
Today we live in a world that is flooded with antibiotics. And although there is concern that bacteria are becoming ever more resistant to them, antibiotics remain an overwhelmingly powerful tool to treat secondary bacterial pneumonia. Early case reports describe these infections in COVID-19 patients, and we have every reason to believe that for many, though sadly not all, antibiotics will provide a cure.
We also have another class of drugs available today: antivirals, which directly target the virus responsible for a disease. There are at least four approved antiviral medications, some given orally and others intravenously. They are not as effective as we would like, but they have been given to a number of very sick COVID-19 patients. Whether those antiviral medications or the antibiotics that are often given in tandem are responsible for successful outcomes is hard to determine. But we have options that were simply undreamed of a century ago.
The advent of modern hospitals, intensive-care units, and medical specialists have changed the response to disease over the past century. During the 1918 influenza pandemic, hospitals offered very few treatments, and many patients were crowded into shared wards where dozens or even hundreds of other people lay coughing, separated from one another by only a flimsy cotton sheet. Victor C. Vaughan, a prominent physician and dean of the medical school at the University of Michigan, left an eyewitness account of the carnage at a field hospital. “I see hundreds of young, stalwart men in the uniform of their country coming into the wards of the hospital in groups of ten or more,” he wrote in his memoir. “They are placed on the cots until every bed is full and yet others crowd in. The faces soon wear a bluish cast; a distressing cough brings up the blood-stained sputum. In the morning the dead bodies are stacked about the morgue like cord wood.” Vaughan was humbled by a plague he could not treat. “The deadly influenza,” he concluded, “demonstrated the inferiority of human interventions in the destruction of human life.”
Today we understand the importance of infection control and the need to isolate patients to prevent cross contamination. We now have intensive-care units where the sickest patients are treated. In some situations, patients may even be plugged into an extracorporeal membrane oxygenator, or ECMO, machine. This box-size unit can temporarily take over the work of the lungs by oxygenating the blood and removing harmful gases. Putting a patient with influenza or COVID-19 on an ECMO machine is a last-ditch effort, the medical equivalent of a Hail Mary pass. But I have seen it work. For the right patient, typically younger, with no other underlying chronic heart or lung problems, an ECMO machine can be lifesaving.
And just as we now have machines with a singular focus, so we have physicians and nurses with expertise in emergency care, intensive care, and infectious diseases. A century ago, there was no such training. The doctor who looked after your influenza might also set your broken bones, deliver your baby, or remove your appendix. We take medical specialization for granted these days, and sometimes complain about the inability of specialists to treat anything outside their own narrow area of focus. But this specialization is precisely what gives the sickest patients the best chance at recovery. From the emergency physician who first diagnoses and treats you, to the nurse who cares for you at your bedside, from the infectious-disease specialist who helps fine-tune your medications, to the respiratory therapist who helps rehabilitate your damaged lungs, specialists working as a team can save the same patient who a century ago would have died, unnoticed, in the corner of a busy and overcrowded ward.
We still do not know how the coronavirus will spread through our communities and how sick it will make us. Early data, sure to be revised, reveal that this disease, like influenza, is much more likely to cause complications in the elderly, those who have a compromised immune system, and those with chronic heart or lung problems. But unlike influenza, and for reasons that we do not yet understand, the coronavirus does not seem to cause serious illness in children. In a moment of dark news, that’s one ray of light.
If the terrible influenza pandemic of 1918 and the current coronavirus outbreak share one feature, it is this: People are terribly afraid. In December 1918, in the midst of the pandemic, 1,000 public-health officials gathered in Chicago to discuss the disease which had by then killed an estimated 400,000 people over three months. They did not know the cause of the epidemic, they had no treatments, and they had little idea how to control its spread. Face masks, which were then being worn by a large portion of the general public, offered no guarantee of protection (and that remains true of face masks today). Many health officials believed that the masks provided a false sense of security. Perhaps that was correct, but there was still a value in providing any kind of security. Chicago’s health commissioner made this clear. “It is our duty,” he said, “to keep the people from fear. Worry kills more people than the epidemic. For my part, let them wear a rabbit’s foot on a gold watch chain if they want it, and if it will help them to get rid of the physiological action of fear.”
The face mask might have offered as much protection as a rabbit’s foot. But it allowed people to feel as if they were doing something proactive, which, even a century ago, was understood to be of great psychological importance.
We can do better. As we wait for the epidemic to abate, social distancing, hand-washing, covering our mouths when we cough, and staying home when we are sick are all important, low-tech measures that we can take to reduce the chances of spreading the infection — and the fear that increases its damage.
_________________
Jeremy Brown is an emergency physician and the author of Influenza: The Hundred-Year Hunt to Cure the Deadliest Disease in History. He is the director of the Office of Emergency Care Research at the National Institutes of Health.